“I had an emotion last week!” I reported to my therapist. “Oh! Tell me?” she nudged. I had been sitting next to Andy, my kind and patient partner, watching the Eagles tromp the Steelers. He had his arm around me, and I dipped my head to rest on his shoulder. The tears started a split second before I registered any emotion. I blinked them away once, twice, and again, trying to tamp down the somatic response as I sorted through the feelings behind them. I turned to Andy and gravely reported, “I have very bad news.” He raised an eyebrow. “I’m starting to feel attached to you.” This was a ridiculous thing to say, as Andy’s been living with me for a few months now. “Good?” he replied. “But you’re going to die,” I whispered, looking at his eyes just inches from mine, “and that will break my heart.”
It’s the end of 2024, almost two and a half years since Mark died and over five years since his brain left most of reality behind. Grief status updates are not a thing, and there’s a reason for that. Grief, at least my grief, is a numbing, erratic, complex, non-linear mess. Like lungs pumping, the air goes into my life and then back out regularly. I have energy; I have none. I want to see people; I want to be left alone. I can plan ahead; I can only live in the moment. “What do you want for dinner tonight?” Andy asks at breakfast. “Why would you ask me such a crazy question?” I frequently reply. It’s difficult to explain why thinking nine hours ahead feels like asking me to plan my own retirement party by dusk, other than to say the obvious: I know that the next moment is not guaranteed. It might be good, it might be bad, it might not happen at all. So I will deal with that moment when it arrives at my threshold, not before.
Andy paused at me declaring his future death during a Steelers’ game. “That’s true. I am going to die,” he said steadily looking at me, “and that will make you sad. But we can enjoy this while we have it.” I nodded and we went back to watching the game.
Grief is memory and memories are like flames; I do not touch them. I generally avoid even resting my eyes on them. If that sounds unhealthy to you, my therapist would agree. The possibility of even a glance at the heart of my grief feels like asking me to lift the gauze on a gangrenous wound. The sight, the smell, the damage – it’s all too much. This makes it difficult for me to carry on light conversations; it makes it difficult for me to carry on any conversations. How do you talk about small things when death looms for all of us? How do you talk about the fact that death looms for all of us? What is there even to say?
My therapist, who would like me to feel more, gently prodded. “Why did you start crying?” “Because I felt safe,” I choked out, “and it could all go away.” She nodded. “Well, that’s everything, right there.” All the pain, the trauma, the loss, the fears.
Over the holidays, my house filled with laughter and love. Alma and their partner Adam, Mark’s three boys, Anya and her partner, Andy and me. I have a bunch of conversation starter card decks in my house; we went through a few of them. “What is your personal version of hell?” Alma read out loud as we sat around a fire, the Christmas tree lights shining. (Don’t you want to come to my house for Christmas?) Those present gamely answered. My first answer? “A small voice whispering in my ear all the mean things I’ve said about (our dysfunctional puppy) Flo.” My real answer was my second one: to witness others suffering.
That’s everything, right there. Life. The beauty and pain of it all. Many days, I’m still frozen in the midst of navigating grief’s glacial melt. The stark whiteness edged by rough grey gravel scree. The exquisite icebergs that can flip at any moment, revealing their giant dangerous blue underbellies. The quiet, the chill, the precarious beauty.
2025 will come, one day at a time. Next to love will be grief; next to grief will be love. Fill the lungs with deep breaths; remember to breathe out.
Mark died 16 months ago. I was struck mute. Words escaped me, and still I find myself functioning moment to moment – sometimes a generous day to day – as I did for so long during his illness. Grief and trauma intertwined to swallow my communication abilities whole.
At this moment, it’s 7:30 pm on New Year’s Eve. Earlier today I moved my bedroom to a new room – again – in my new house, as renovations continue. I’m lying in bed, my mattress on the floor, in the smallest room in the house. It feels like a cozy nest. A scented candle is lit, “Frasier Fir,” and lime Bubly is at my bedside. Duppy is tucked into her winter curl, and Flo and Bob are splayed in the nearby doorway. Matthew is out with friends. I am alone, but as always, I do not feel alone. I am accompanied by memories and thoughts that swirl relentlessly in my mind.
Mark died. He used to be alive, and now he is not. Part of him is in my room, on my bookshelf. Ashes. Part of him is in a cemetery 15 miles away. Part of him is in pottery glaze, in the icy waters around Iceland, in the Canadian tundra, on his way down the Ohio River. His photo smiles at me from the shelf. His name marches on in typeface on papers on my desk. One of his sons has their dirty laundry on the bed floor down the hall, and my Christmas tree holds ornaments from the childhoods of three orphaned boys.
What is grief? This thing I’ve been trying to understand, live with, integrate, endure and befriend.
Mark left us in August 2022. All of time since has been some version of a blur. For much of that time, and as frequently as possible, I was supine, prone, fetal. I lay down at any chance I could get. During a lull in parent-teacher conferences, my colleague covered me with a blanket when I laid across the tables. If I needed three naps a day, I took them. There are still days like that. “Your body needs rest,” my therapist affirmed. It did, and it does.
As per the norms of life, it’s only after an experience that you more clearly see what occurred, and for sure I can now see that the amount of trauma I absorbed was, frankly, massive. “You’ll never forget the things you see,” Mark’s sister told me in his first stint in the ICU, as he gagged up blood while trying to rip his intubation tube from his mouth and she guided me out of his room. She was exactly correct. It all replays now, like a film I’m watching of someone else’s life. “What do you feel?” my therapist asks. “Nothing. No emotion,” I say. In waking hours, that is most often the case. When I sleep, my emotions fight to be heard. Last week, I dreamed that Mark was gasping for air, unable to get a breathe, mouthing, “Help me!” In my dream, I looked over and saw the boys and yelled, “Look away! Don’t watch!”
And then, in my dream, I watched him die.
Because in my life, I did watch that.
We saw so much.
Occasionally, rarely, in the light of day I find that a feeling breaks through. A song comes on the radio, a memory abruptly pushes to the forefront, and I’m struck again with the facts: Mark died. He died after three years of a horrible illness that left not much more than the stubborn core of his being for me to care for, nurture and love. I held on tight, watched, learned, instructed, was led, endured, navigated, and felt helpless through every moment of it. It was a horrible, horrible experience. It was pure love, and it was a nightmare.
Now, I just try to get through every day. “Do you have family traditions you observe around the holidays?” an acquaintance asked a couple nights ago. I stuttered to answer, taking a quick mental scan of how unstable my family has been over the years. And that’s because of Mark, his life and his kids’ losses, and because of my life before Mark. Divorce and it’s own set of traumas. It’s hard to keep traditions with such constant morphing and disruptions of norms.
Here’s what I do now. I take care of my dogs. I drive forward with decisions about house repairs. I teach students about the natural world. I love all my kids. I navigate changes, as the matriarch of the family. In the year and a half since Mark died, Matthew started college, Michael moved to Arizona, Ben moved out. Adam graduated law school, Alma quit and did six months of self-care and then gained a job, Anya built me raised beds and is working with my contractor on my house repairs. I traveled to northern Manitoba to see the Northern Lights. Alma, Adam and I explored the endless wonders of Iceland. I dug into cowboy life in Texas with my brother and his wife, and I drove to Chicago for an amazing visit with old friends. I sold the family home in Upper St. Clair and moved into the City of Pittsburgh. I’m working on renovating this house to make it a home. I gained an amazing housemate who is already a part of this complicated, messy, perfect family.
I am doing so much, and somehow, someway, I feel that I am exactly where I was 16 months ago. Frozen in the moment of Mark’s passing.
I have written almost nothing in all this time. It’s felt impossible, like it might feel to look at a singular stone and know it’s the first stone to move to build a retaining wall. I’ve felt like I want to write about Mark’s actual passing, the sacred experience of being with him as he crossed the threshold from here to there. I will someday, I’ve promised myself and Mark that. And so far, every day has not been that day.
Grief. What is grief? Hope. What is hope? Loss. Trust. Grounding. Future. Possibility. Stability. Safety. What are all these things? I’m a year and a half past the loss of Mark, and here’s my honest answer. I don’t know yet.
It’s 8:00 pm on New Year’s Eve. I’ll think about it more tomorrow.
Young Matthew, the last of the herd, turns 18 tomorrow. This feels heavy to me, so maybe today was not the day to be wading through Hrehocik family documents…mortgages and cars and insurance from decades back. What to keep, what to discard, as Mark and Kristen’s remaining family archivist?
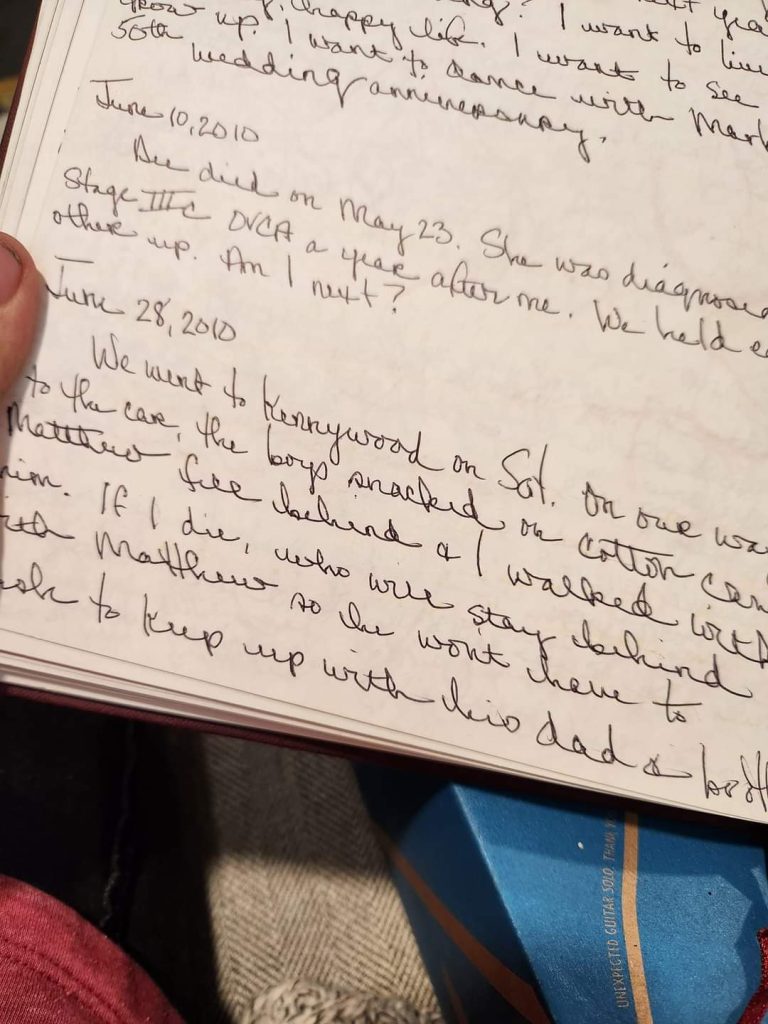
I came across one of Kristen’s journals. She journaled a lot from the time she was a teenager until her death. This particular journal covered the last part of her cancer journey. Her cancer, ovarian, was bad from the get-go, and she fought it bravely and beautifully for six years. I only read a few entries: her last in the summer of 2012, and this one from June 28, 2010. In both, she worried about dying. In this one, she focused her fears on 5 year old Matthew. Mark and Kristen had taken the kids to Kennywood that day, and Matthew’s little legs couldn’t keep up with his dad and brothers’, so Kristen fell behind and walked with him.
“If I die, who will stay behind with Matthew?” she wrote afterwards.
Me. It’s me, Kristen. I am staying behind with Matthew, and I always will. You raised a beautiful, kind, funny, patient, thoughtful, intelligent young man. I wish you were here, with Mark, to celebrate him.
Real talk here from the widow-who-shall-not-be-judged-because-grief-is-an-individual-thing: tomorrow I bury Mark.
Well, the part of him I’m going to bury, anyway, as the boys want to spread some of his ashes where their mom is spread. Which means that today, I had to do the task I’d been putting off: dividing the ashes. I had gotten stuck on the idea of closed and open systems. (Career problem.) Once that bag was opened, there would be no chance of not having wastage. Some of Mark would drift away, lost in the floorboards of the house or wherever the wind would take him. I forced myself to do it anyway. I took the plastic bag filled with Mark outside, cut off the zip tie, and started scooping out Mark ash, Mark bone, and either what is part of his knee replacement or part of the crematory machinery that fell onto his body (I think the former). I filled two empty pill containers for absolutely no reason (rainy day mentality?), one gallon-size ziplock bag for the future spreading activity with the kids, and then resealed the original bag with a new zip tie and put it in my car so I don’t forget to take it to the cemetery tomorrow (widow-brain is no joke.).
There was wastage; how could there not be? I wiped my hands off on my kale plants and the sweatshirt of Mark’s that I am wearing. I’m letting the little table I worked on, now covered in DNA-infused Mark powder, to sit in a sunny, windy spot to let nature move him wherever she will. (Bob has decided to guard it.)
The day is stunningly beautiful, the Steelers must be losing judging from the neighbors screaming on their patios, and I feel sad but I am okay. Mark’s not in that ash, anyway. He’s with me, in my heart and mind. Just like before, I am carrying him. Love. Isn’t it amazing?
I think about it on average about every minute of every day. Sometimes it hits me with surprise, and sometimes I am just turning it in my head like an unfamiliar object I am exploring with my hands. It’s been 44 days, and his death feels like it was both yesterday and long ago. It’s shocking, still, that it will be true later today, and tomorrow, and forever.
At 53 years old, I’m fortunate to say that I’ve never had someone close to me die. Because of that, nothing about this experience is expected. Heck, Mark dying was not expected. (I’ll write more about that at some point. I am not ready.) For the first few weeks after he died, I took to my bed, climbing out just to do the necessary things, like going to work, interacting with the kids, and dealing with the depressing paperwork that death brings. I’ve slowly been regaining energy, but I am still finding my center in the simple act of resting. Looking in the rear view mirror, I can see that for the three years of Mark’s illness, I never truly rested. Every moment of every day was shaped by taking care of his every need. I woke when he woke. I slept when he slept, the kind of terrible sleep a new parent has while keeping one ear attuned to the breathing of their baby. Now my body relishes the simple act of laying in bed for as long as I need, as many times a day as is needed, the dogs nestled next to me, my bedroom chilly and the blankets piled high. None of those things in the last sentence were happening before. I am living in loss and in peace.
Grief is exhausting work. My brain is constantly shifting around the facts and feelings. I feel deeply respectful and protective of the process, like I am parenting my brain-child. Does she need sleep? Let her sleep. Does she want to take a walk? Yes, let’s do that. My brain-child likes lattes, Netflix, and quiet. She is sad, of course, and that makes complete sense. Sometimes she feels content, and that’s surprising. She is living in the moment, still, having been highly trained to stay in the present with Mark.
I came to this place of Mark leaving the earth with exactly no construct around death. Thoughts, opinions, considerations, yes. But arriving here, in a painfully non-theoretical place, has opened up thought processes that I have never explored. The most immediate has been, of course, where is Mark? He was here, and now he’s not. When Mark died at hospice, my friends and family stayed with me, with him, until I felt a separation between Mark’s body and spirit. I was sitting next to his body; that’s all that was there anymore. I could leave that room, leave that body, because Mark had left it, too.
Weeks later, my living room a sanctuary decorated in dried flowers and twinkle lights strung up with sympathy cards, I continued to consider this: where is Mark? Before he died, I always knew exactly where he was: on the couch, in bed, at memory care. He was gathered in one place. Was he now fully absent? Or with no body, was he more fully present than he ever could have been? Then any of us can be, bound to our flesh and bones?
My therapist encouraged me to go out for a hike. I returned to the park I’d so often walked when I was getting breaks from watching Mark. The day was overcast, the wind tossing the treetops, the wetland water rippling, the geese and ducks bobbing and feeding. I down sat on a bench amidst the swirl of energy of life all around me, and I wept. Where was Mark? Looking across the landscape, something came flying towards me, landing under my legs. Peering down, I watched as a large praying mantis swiveled its creepy little head to look up at me. My tears turned to laughter. Mark was an engineer and worked in numbers. He made exactly one sketch for me, ever, years before when we were dating: a praying mantis. If Mark was going to send me a little message from the spirit world, this seemed like a Mark-way to do it. I watched the praying mantis for a long time, finally saying goodbye to it, carrying a dose of happiness and peace with me as I walked out of the park.
I know that meaning-making is part of the deal of being human. And I believe that the creation of personal narratives is just that – personal. I am experiencing Mark’s death as a creative process unlike any I’ve ever explored. Mixing all the things of my life into the soup of my electrochemical brain – nature and art and religion and science – and the most beautiful thing has merged as my personal truth: I get to make sense of my world, and if my construct helps me, and if it doesn’t hurt others, then I believe it is good. It is GOOD. In that moment with the wind whipping and the smell of autumn leaves decaying, staring at that praying mantis, I chose to believe that Mark was, indeed, everywhere now. He’s with me as I write this early in the morning laying in bed. He’s with me on my commute to work. He’s with me when I go to the movies, or out to dinner, or sit by the fire on my patio.
Mark’s body is not here anymore, and in that I miss him all the moments of my days. If I could choose, I’d still be taking care of Mark everyday, keeping him safe and feeling loved. But have I really lost Mark? I think no. The gifts Mark gave to me through our long, difficult, love-filled journey stay with me. I can still talk to him, still be with him, in ways I don’t really understand. And I’m okay with that. I can continue to turn it in my hands, heart and mind, this new experience with life, these burgeoning thoughts and explorations. I can also just let it be. Either way, I will be okay.
My loving, kind, quiet, funny, positive, gentle, confident, and smart husband, Mark Joseph Hrehocik, crossed over the threshold of this world to the next on August 25, 2022, at age 59 from dementia caused by sinonasal undifferentiated carcinoma and treatment. Born in and faithful to his Mon Valley roots, Mark was the epitomized Pittsburgher, holding only two jobs in his life: working a game booth at Kennywood Amusement Park and enjoying a 36-year career as a mechanical engineer at Bechtel Bettis Atomic Power Laboratory. A proud Slovak and the youngest of seven raised in Glassport, PA, Mark believed in both the simple joys of life and in working hard while pacing oneself. Mark loved mentoring younger engineers, spending time with his three children (Michael, Ben, and Matthew) and two step children (Anya and Alma), a solid round of golf, a lunchtime run on a hot day, and a poker game with friends. He could identify which play a Shakespeare quote was from and sing every lyric to songs from Bob Dylan to Bob Marley to REO Speedwagon. His two favorite books were Les Miserables and Ball Four.
Predeceased by his first wife Kristen, stillborn daughter Kayleigh, parents Michael and Pauline (Terek) Hrehocik, and sister Tish, Mark knew sorrow. He drew from this deep well, practicing compassion for others, a seize-the-day zeal for life, and the wisdom of knowing that sitting outside enjoying a sunset has just as much value as accomplishing any task. We learned from each other the depths of love in the hardest of times. We were grateful for the good days and found joy tucked into the folds of the bad days. We felt fortunate for the time we had together.
Mark and I knew each other through nearly equal years of sickness and health. Mark was always insistent that he was going to live forever. He would have given anything for one more day with Michael, Ben, and Matthew, and to get that—just like their mom did—Mark gave everything. I wish he had been right, but Lord, did he fight a good fight.
My Mark now sails through time and space, launched into the unknown and unknowable, a brilliant soul and spirit untethered from the confines of our small and beautiful world. In addition to me (his wife, Diane Reckless), Mark is survived by many who loved him: his three sons, Michael, Ben, and Matthew; two step-children Anya and Alma; four sisters, Paula Roche (John, dec.), Teena Culbert (Roy), Jane Clampitt (Henry), and Marcia Uziel (Don, dec.); a brother, Michael Hrehocik (Vickie); nieces, nephews, friends, and a huge and immensely generous community that rallied to support our family for the past three years. Please join us for a celebration of Mark’s life at East Liberty Presbyterian Church, 116 S. Highland Avenue, Pittsburgh, on Saturday, September 10, at 10:30am. Reception to follow in the church social hall. Please feel free to send all the flowers; Mark loved them. Memorial donations in Mark’s memory may be made to the Light of Life Rescue Mission, 913 Western Avenue, Pittsburgh, PA 15233. Please visit the funeral home website (www.dalessandroltd.com) to leave a personal message of condolence for Mark’s family.
Apparently the Rainbow Bridge is for animals, not people, but I like to think that Mark passed over riding on a glorious spectrum of light energy, has found his mom, dad, sister, and first wife, Kristen, has met his baby daughter Kayleigh for the first time, and is petting their dog Seamus. I hope he is laughing, singing, and organizing a softball game. I hope those that went before him gave advance notice to the angels that Mark likes to do things his own way, is deeply compassionate and kind, and may not follow every heavenly rule to the exact letter. Mark Joseph Hrehocik passed away at 12:55am, August 25, 2022, eight hours shy of exactly 10 years since Kristen died. He was surrounded by love and laughter and tears. He was and will always be cherished. Service to be announced.
Dear Friends and Family near and far, neighbors, community members, and virtual strangers who have appeared and woven themselves into a cherished framework of online support: My beautiful Mark is leaving us. He was diagnosed in August 2019 with sinonasal undifferentiated carcinoma. He is cancer free, but the accumulated damage from tumor and treatment has become too much for Mark to endure. Ultimately, radiation causing encephalomalacia (brain damage), and the encephalomalacia causing seizures that are drug resistant, is the probable cause. His body is simply slowing down and stopping. He is comfortable and being cared for by a wonderful team. Everyday, I tell Mark over and over the best thing I know to say: he is good, and he is loved. Every person reading this has helped us in some way, even if just by joining us from afar on this journey. Thank you. There have been many terrible times and many joyous moments and so many peaceful hours of contentment and love. I am grateful for the three bonus years Mark and I had together. I will keep holding his hand until the time comes when his spirit is ready to soar. With love, Diane
I started a blog post in June that looked like this:
“Death by a Thousand Cuts”
What Mark can’t do:Regulate his eating. Have a conversation. Use a phone. Understand a clock. Track time. Understand his limitations. Remember conversations. Remember for 10 minutes what he’s done, where he’s been, what he’s eaten.
What Mark can do:Feed himself. Dress himself. (Kind of – got lost putting on his pants today. Forgot to put on a shirt.)Toileting.Grooming? (Not sure.) Bathe? (Not sure.) Mobility (in wheelchair).
Things had changed so dramatically and quickly with Mark over just a few weeks; I was simply trying to organize my observations. In May, Mark could go outside by himself, retrieve the newspaper, and read it. After his seizure and fall in June, resulting in a broken kneecap and a return to the wheelchair lifestyle, Mark never fully came back up to his previous cognitive baseline. He was unpredictable in new ways. Not all of them were bad: he started parking himself in front of the pantry and grazing on random foods. He decided against the container of nutritional yeast he opened, but happily polished off bags of Doritos and spoonfuls of peanut butter. His persistent aim of finding and consuming any alcohol in the house simply stopped. Non-alcohol calories were welcome, so I was happy with this change, except that it represented some kind of invisible shift that was out of character and therefore might not good. And then some of the changes were obviously not good: he wore dress pants one day because he “couldn’t find” his other pants. If I didn’t turn on Jeopardy, he didn’t remember our nightly habits. He stopped reading.
The “Death By a Thousand Cuts” blog draft title referred to both of us. I dug in and tried hard to keep up and interpret the painful and reductive changes. Mark was going deeper into himself, less able to answer simple questions or even finish a sentence that he might start. Lying next to him at night, I felt his small muscle spasms that indicated seizure activity. His many meds were not keeping up with the electrical storms flaring in his brain.
I read a lot about seizures and brain damage. I watched an excellent 90-minute-long video tutoring med students on the topic of seizures to prepare for their boards. I discussed what was happening with Mark’s doctors. The answer, in short, was we don’t exactly know, and we can never know. Scans showed no tumor growth or other emergent problems. The remaining causes for his decline — seizure meds dulling him out, or brain damage from the seizures — were equally possible, and completely unknowable. The only way to find out would be to reduce his meds, increasing the chance for seizures. And since his seizures are very dangerous, we cannot do that. Therefore, nothing could be done, other than the last ditch option of 50/50 success with the vagus nerve stimulation (VNS) surgery planned for late July.
In late June and at the point when Mark started unlocking the gate at the top of the foyer steps and announcing he was going out for a bit, I decided I needed a break from the 24/7 stress. As caregiver rhythms can align with the cared-for, I sensed my reserves rapidly declining at a rate commensurate with Mark’s changes. I booked him for a two-week stay, starting July 5, at the same senior living facility he had stayed in last September.
Early on July 4, the day before he was scheduled to start his respite stay, Mark again tried to leave the house. “Where are you going?” I asked. “For a walk.” He was hovering at the top of the stairs. “I’ll go with you,” I replied. I carried his wheelchair down the steps as he carefully held the railings and walked down, one step at a time. At the bottom, Mark climbed back into his wheelchair and started rolling towards the car. “I thought you wanted to go for a walk?” I said. “A walk? No, I want to go for a drive,” he said firmly. He kept rolling to the car.
Okay.
I loaded up the wheelchair and Mark, and I headed south on Rt. 19. I put my “Mark’s Happy Place” Spotify playlist on the radio, and we sang along together to rock and folk from forty years ago. Bob Dylan, Journey, REO Speedwagon. I thought Mark might want to visit one of the nearby lakes we frequent, but he wanted to keep going.
An hour later, I pulled into Wheeling, West Virginia. I’d only been there once before, years ago. I located a waterfront park along the Ohio River, unloaded Mark, and pushed him along the walkway. We looked at war memorials, train line memorials, and a tug boat slowly pushing coal downriver. We watched a stage being erected for an evening concert. Mark was mostly silent. The air was still early-morning cool when we got back in the car and headed to nearby Oglebay Park. We took in the beautiful gardens, and then drove onward to an outdoor BBQ place down the road. Mark ate every bit of brisket, including the bits of fat that we both had trimmed off.
Leaving the restaurant, Mark stayed perfectly still as I stopped his wheelchair next to the car. He looked completely drained.
“Lock your wheelchair,” I instructed. He did.
“Get into the car,” I coached. He did.
“Put on your seatbelt,” I prompted. He did.
Back home, Mark seemed perfectly happy but exhausted. We had had a good day, but Mark hadn’t really reacted to most of what we did. I’m not sure he even knew where we had gone. And by dinner time, he had forgotten we had gone anywhere at all.
The next day, I drove Mark to the senior living community. I simply explained he was there for rehabilitation and rest; he accepted it without a word. Many of the staff people recognized him from his stay last year and greeted him by name as we reached the locked third floor memory care unit.
When I returned to visit the next day, I found Mark sitting outside on the enclosed patio, enjoying the sun. He appeared utterly content; the food was “good!” and the people were “nice!” We visited for a while until he got tired. I pushed him back to his room, tucked him into bed under his fleece Steelers blanket, and gave him a kiss goodbye.
Then I went home and cried. And I continued to do so for days while encountering one serious thought after another. Mark was safe and content in a facility staffed with people acting as a team to care for him. I wasn’t alone in caring for him, as I usually am, and that felt like an immediate relief. Taking a step away from the boulder I had been pushing up the mountain helped me acutely feel how very heavy it was.
Questions and thoughts I didn’t even know I had started to rise to the surface. I had space and time to think. Stepping out of the box of daily tasks related to caring for Mark, I found there was a lot to consider.
The first decision I made was based on the most primitive instinct: an immediate, clear, gut feeling. Sitting quietly that second day on the patio with Mark, the white lattice and flower pots bright in the sun, two red-tailed hawks soaring overhead and the unit cat snoozing nearby, I looked at him and thought: I can’t take him back to the hospital. I cannot. The VNS surgery was elective and outpatient, and therefore much less scary than, well, EVERY OTHER SURGERY that Mark has had. But there is anaesthesia, which Mark is historically not great at handling, and the chance for infection, and the every-three-month monitoring of the device driving us back to the hospital more and more. Also the little part about there being a mere 50% chance of the VNS working, and “working” meant reducing his seizures in frequency and intensity by, optimistically, 50% at best. I’d been so sure, just a month earlier, that this was worth trying. Now, seeing Mark at peace, his body being as whole as it can be, his brain as good as it very well will likely get, the opposite seemed clear.
The compassionate choice would be to not put him through another surgery, and especially one that would cure nothing.
I let those thoughts sink in for two weeks.
They didn’t change.
I canceled the surgery.
The second thought that popped unexpectedly into my head after I dropped off Mark was this: he was exactly where I’d want him to be if I could not take care of him at home anymore.
He. Was. THERE.
This is the facility where my friend has nursing privileges. Another friend, a retired colleague from school, messaged me to say her dad is in the same unit. She was visiting with Mark during his respite, and reporting to me he was doing well. The facility is one mile from our home. It’s small, well-kept, and safe. We’d had a good experience with him there last September.
I worked with these thoughts for a couple weeks. I thought about the losses I already had endured in this journey with Mark, and how both his cognitive decline and his physical body being away felt like unearthing new levels of loss. I felt deep grief. I missed him. I missed the physical him being with us in the house, shaping my days. I missed the Mark I cannot have back, the one before he was battered by cancer and treatment. I’d always assumed that keeping him at home was the absolute clear and best decision for him. How could it not be? I talked to friends and family. One person said, “At this point, what is safest for Mark is the best decision, and it does not seem like it’s safe for Mark to be at home anymore.” I wasn’t sure I agreed. Another friend said, “If you decide to keep him there longer, remember you can always change your mind.” I found resources to read, podcasts to listen to, and kept open to observing my feelings and thoughts as they fluctuated throughout my days. I tried to imagine the possibility of it being the loving decision to keep Mark in memory care. Was I really not able to keep him safe? Could I be a good partner to Mark if I didn’t keep him at home? What was best for Mark? What was best for the boys? What was best for me?
After one week at home, visiting Mark daily, I drove east for a family vacation. On the way into New Jersey, I had a phone session with my therapist.
“Am I being impulsive?” I asked after explaining the possibility of extending Mark’s stay.
“No,” she said.
“Am I being selfish to be to feeling like I can’t do it all to keep him safe and at home forever?” I asked.
“No.”
I barely whispered my final question: “Can I be done? Did I do good enough?”
“Diane,” she said, “you did more than good enough.”
I extended Mark’s stay by two weeks to see how that felt.
It felt sad. It felt like loss. And in my core, I detected something else. It felt right. It felt like it was time. By all metrics, Mark was doing well. This was coming from a tragic place: his cognitive function was now so poor now that he was not tracking where he was, why, or how long he had been there. And without tracking the hours in the day or the days passing, or a conversation or even a full thought, Mark could simply be.
Mark was always good at that, being present in the moment, and now that is where he truly lives the most. He’s often napping, or on the patio, or accepting staff guidance to play bingo or UNO. He laughs and smiles when they play a game of toss with a beach ball. His answer to how he’s doing is still, often, a solid, “Great!”
And so here we are, friends, a place I did not know we were going. Mark now lives one mile down the road, in a locked memory care unit. That’s where he will stay unless something I currently can’t envision — but am open to — changes. I am living my days mostly as I had before. Exercising, reading, taking care of household things and the boys. Waiting for the other shoe to drop, which is a hard habit to break, and being so glad it’s not.
I visit Mark every day. He never asks to leave, he never asks how the kids are, he never seems sad or uncomfortable.
I’m choosing to look at this as the next stage in a story about love. And that is a conscious choice, in a story that could be defined more by loss than love. There will be a lot of beauty in this stage, too, woven in with sadness. We will continue to create a tapestry of exquisite beauty born from this complicated life and love. It will be clearer from the long view, and on hard days, I will remind myself of that.
This morning on my way into the facility, I stopped at the front desk to make sure they had posted Mark’s picture, as we had discussed. A few days earlier, every staff person I encountered had made sure to tell me, with surprise and wonderment, that Mark had achieved a rare feat; he had escaped the locked third floor and was found wandering on the first floor. He was walking, having forgotten – as he does – that he uses a wheelchair. When I heard the news, I talked with staff and made sure they had a plan for how to keep him safe. And then I allowed myself to feel a surge of joy that underneath all the damage, deep in the hidden corridors of his brain, he’s still my smart and clever Mark. It was delightful and funny. That’s my guy, still the troublemaker.
It was 8:15am when I got off the elevator and walked into Mark’s room. He was sound asleep. I woke him up and brought him to the dining room for breakfast. I greeted the care team and residents I’ve come to know by name, and they greeted us by name, too. I made conversation with Mark and a pleasant couple living on the unit, Peggy and Paul.
After Mark finished his scrambled eggs, bacon, sausage and coffee, I pushed him back to his room and directed him into the bathroom. He brushed his teeth, twice, because he forgot within minutes that he had already done it. I turned on the shower, adjusted the water temperature, and instructed him to get undressed. He looked at me, trying to process, and instead unlocked his wheelchair. I relocked it. “Take off your sweatshirt,” I coached, gesturing to demonstrate. He unlocked his wheelchair again. I relocked it. I pulled his sweatshirt off, revealing that he was, in fact, sporting two sweatshirts in addition to a t-shirt. This clown car of clothing continued. He was wearing, between his two feet, five socks. He had two pairs of pants on. Why? He couldn’t tell me.
After his shower, he shaved one side of his face and I shaved the other. I rubbed lotion gently across his very dry face and forehead.
“What do you want to do now? Sit outside, or take a rest?” I asked when we were finished.
“A rest,” he said, transferring from his wheelchair into bed.
I kissed him goodbye, and then I drove home to figure out how to pass my day.
This isn’t the end of the story. It’s the next part, which includes Mark, my husband, living in memory care, and me, his wife and caregiver, taking care of him in new ways.
Alma, discussing Mark not living at home anymore, asked me how I will adjust. “Well,” I said, “I don’t think I’ve let my identity get too wrapped up in being a caregiver.” Alma let out a guffaw. “Mom. Your Instagram name is ‘dianelovesmark.’” Point taken.
We will have to just keep living this life and see.
I’m lying next to Mark in bed. It’s the middle of a hot summer afternoon. Mark’s shirt is off, and I’m considering his stubborn body, the body that has taken so much and keeps going. There are various portals, now sealed. The small puncture in his abdomen where the feeding tube brought him back from the grip of death in the winter of 2020. The scar on his throat where a trach brought oxygen to his lungs and removed pressure from his skull graft in the summer of 2020. There is the scar draped across his head, ear to ear; the line they drew once and then used as their guide for multiple returns into his skull and brain. The scars on his leg and scalp from drains. The 18-inch scar on his leg from the harvested quad muscle in the spring of 2021.
“You didn’t really say too much about your feelings,” Kim told me after reading my last post. “But that makes sense,” she quickly added, “you had a lot of information to convey.”
She’s right. I’m not living in my emotional life right now. Sometimes I can, and at those times I do. Sometimes my emotions are a safe space, a gentle summer air current keeping a butterfly aloft. Sometimes they are as rough as the velcro strips holding Mark’s leg brace firmly in place. Any tug could cause a dislodging that feels like it would be a catastrophe.
My Mark is gone again, and as usual it happened suddenly, without warning. Now he lives in a state that is seemingly a combination of brain damage and drug haze, and the line between the two is dashed and wonky. A weaving of brain tissue, electricity and chemicals that feels more soup than solid.
My Mark is gone again, and it happened in a flash.
I feel alone.
I have decisions to make, the worst kind of decisions, while taking care of a Mark that can turn on a dime, wake up on a lark, forget that he uses a wheelchair again, and head down the steps. “Where are you going?” I ask. He doesn’t know. He can’t answer. He doesn’t answer.
I have no idea how to make these decisions. They are: keep Mark on the medications and therefore keep the seizures as controlled as possible; take him off the sledgehammer medications so that he’s more alert in his life; consider surgery to treat the epilepsy.
When I do the math, which I am doing in an endless mental loop everyday, I always come up with this: No Good Decision.
Mark does not have a terminal diagnosis. He is alive and living with a complement of disorders, diseases, syndromes.
“Do you know what ‘chronic small vessel ischemic disease’ is?” my friend Tory asked. I had sent Tory screenshots of a scan report from after Mark’s seizure and fall two weeks ago. I did know, but only because I had looked it up. Has any doctor told me Mark had this chronic disease? Nope. Not one, ever. Did I dwell on this for a second? Nope. I moved on. What did I need to understand about it? It’s a precursor to dementia and strokes. Info received; move on, Diane, move on.
As I said, I’m not living in my emotions. Which is clearly a short-term strategy that will not hold up long-term. There’s a lot to feel about the current reality. Is the Mark I’ve had for the last nine months, quite mentally recovered, present, funny, connected, kind, loving, gone for good this time? Are there ways to uncover the layers of medication fog safely, to see what Mark is under there? Who can help me answer those questions? Who can help me figure it out?
See, I’ve gone from emotion to labor, once again. Task, task, task.
I’m sad. I can tell you that. I’m tired, at three years into this. “I wish so very much for a dollop of joy to land in your lap,” Kim texted me yesterday. Very unlikely, I replied. I can’t even envision what form joy could take. What would joy even look like right now?
Luckily the work is ample. I simply navigate through my days moving in tandem with Mark’s whims. He’ll suddenly put on his baseball cap and shoes. “What’s next?” I’ll ask. He may or may not answer me, and then I just follow him wherever he rolls.
Someday I may be the driver in my own life again. I sure hope so. For now, I navigate the ribboned stream of leading and following, not quite sure where we are going or who is actually in charge. The line, the path, extends to the horizon.